Background
Asymptomatic atrial fibrillation (AF) is associated with an increased risk of stroke. The yield of serial electrocardiographic (ECG) screening for AF is unknown.
Methods
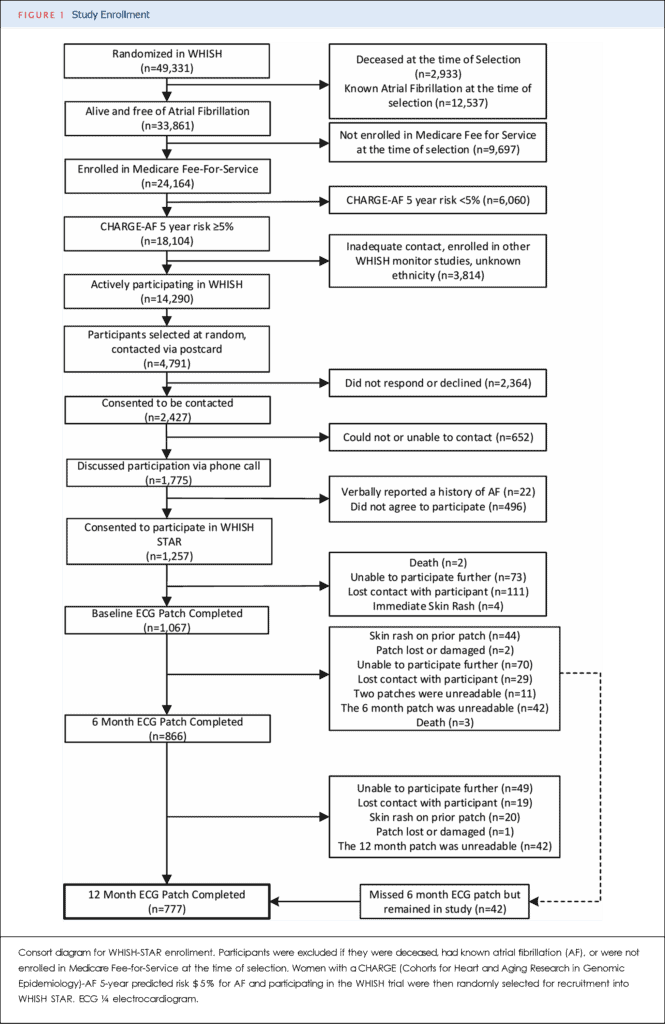
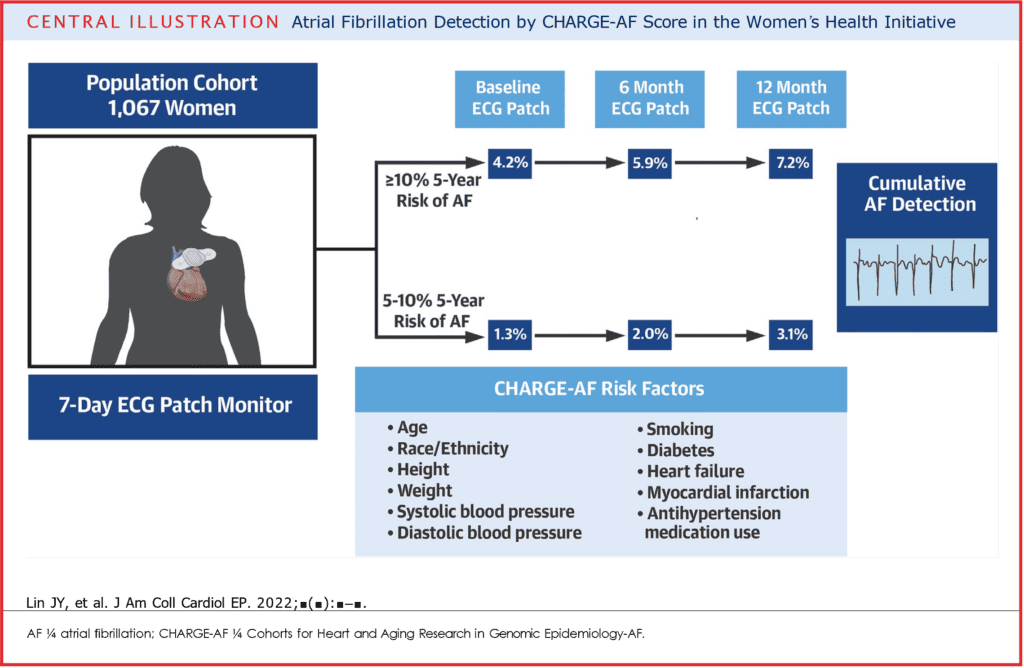
Postmenopausal women with a 5-year predicted risk of new-onset AF ≧5% according to CHARGE-AF were recruited from the ongoing WHISH (Women’s Health Initiative Strong and Healthy) randomized trial of a physical activity intervention. Participants with AF at baseline by self-report or medical records review were excluded. Screening with 7-day ECG patch monitors was performed at baseline, 6 months, and 12 months from study enrollment.
Results
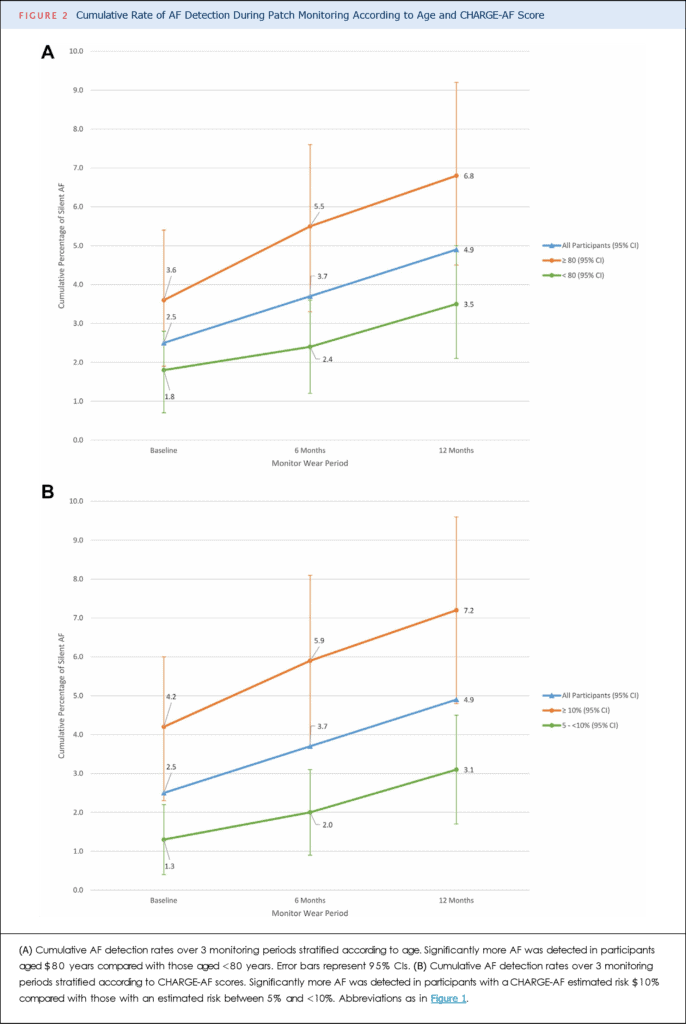
On baseline monitoring, 2.5% of the cohort had AF detected, increasing to 3.7% by 6 months and 4.9% cumulatively by 12 months. The yield of patch screening was higher among participants with a higher (≧10%) CHARGE-AF score: 4.2% had AF detected at baseline, 5.9% at 6 months, and 7.2% at 12 months. Most participants with patch- identified AF never had a clinical diagnosis of AF (36 of 46 [78%]).
Objectives
The aim of this study was to determine the frequency of AF detected by serial, 7-day ECG patch screenings in older women identified as having an elevated risk of AF according to the CHARGE (Cohorts for Heart and Aging Research in Genomic Epidemiology)-AF clinical prediction score.